Recommendations For An Effective WPV Safety and Health Training Program That Is In Alignment With Joint Commission and OSHA Guidelines
Workplace violence (WPV) in healthcare is well documented. Out of all workplace assaults in the United States, fully 75% of them occur in healthcare and social service settings (OSHA — (Occupational Safety and Health Administration).
This shouldn’t be surprising given the prevalence of the following WPV risk factors in healthcare settings that have been identified by California OSHA and NIOSH (National Institute for Occupational Safety and Health).
Employees who:
- Have contact with the public
- Work alone
- Work late at night or during early morning hours
- Perform duties that put them in conflict with others or that could upset people
- Deal with people known or suspected to have a history of violence
- Have a mobile workplace, deliver passengers or goods, and must enter areas with a high crime rate
- Exchange money with the public
Workplaces that are:
- Often understaffed
- Located in an area with a high crime rate
Anyone who has ever worked in healthcare (e.g., hospitals, residential treatment, clinics, community care, home care) has come to accept that these risk factors are, largely, just part of the job. Therefore, it should be no surprise that workers in health care settings are four times more likely to be victimized than workers in private industry (Security Industry Association and IAHSSF Foundation).
What Is Workplace Violence?
The Joint Commission’s infographic — Take a stand: No more violence to health care workers — lists the following forms of violence to healthcare workers: biting, kicking, punching, pushing, pinching, shoving, scratching, spitting, name-calling, intimidating, threatening, yelling, harassing, stalking, beating, choking, stabbing, and killing.
The U.S. Department of Labor “defines workplace violence as an action (verbal, written, or physical aggression) which is intended to control or cause, or is capable of causing, death or serious bodily injury to oneself or others, or damage to property. Workplace violence includes abusive behavior toward authority, intimidating or harassing behavior, and threats.”
OSHA addresses employee complaints of workplace violence and assesses employers based on OSHA’s General Duty Clause, Section 5(a)(1) of the Occupational Safety and Health Act of 1970.
“(a) Each employer shall furnish to each employee employment and a place of employment which are free from recognized hazards that are causing or are likely to cause death or serious physical harm to employees”
As further evidence of the problem of workplace violence in healthcare settings, of OSHA’s inspection resulting from an employee complaint, more than 65% over the last few years involve the healthcare industry. And, given the prevalence of the risk factors listed above and the number of workplace violence incidents in healthcare, it is likely that OSHA identifies some level of hazard with every inspection.
It is important to understand that, even if OSHA identifies a hazard, they cannot cite a healthcare organization just for not having a WPV program — since no specific workplace violence standard exists. Instead, OSHA can only cite an organization if OSHA can show that a hazard abatement action would have reduced the likelihood of “death or serious harm.” Therefore, even though OSHA doesn’t have a specific workplace-violence standard, employers can protect themselves from a citation by having a strong WPV program.
The goal for healthcare organizations should be to have sufficient elements of a WPV program in place to minimize the chance that OSHA will be able to show that actions could have been taken to materially reduce whatever hazard they identify during an inspection.
Other reasons to have a strong WPV program are:
- Protect the safety and well-being of employees, patients, and visitors
- OSHA is in the process of developing a workplace violence standard for healthcare settings
- Several states (CA, CT, IL, MD, MN, NJ, OR, NY) now require an employer-run healthcare violence program and many others have laws designating penalties for assaults that include nurses (American Nurses Association — Workplace Violence)
 In absence of a standard, OSHA has published Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers – 2015, which identifies these five building blocks for an effective WPV prevention program:
In absence of a standard, OSHA has published Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers – 2015, which identifies these five building blocks for an effective WPV prevention program:
- Management commitment and employee participation
- Worksite analysis
- Hazard prevention and control
- Safety and health training
- Record-keeping and program evaluation
What Should be Included in a Workplace Violence Training Program?
At Vistelar, due to our trainer’s 30-plus years of providing conflict management training for healthcare employees, we often are asked what should be done relative to the fourth building block: safety and health training.
To answer this question, we encourage our clients to first review what the Joint Commission and OSHA have to say about workplace violence training.
The Joint Commission’s latest publication on this topic — Physical and verbal violence against health care workers (Sentinel Event Alert Issue 59, April 17, 2018) — says this on page 6:
“Train all staff, including security, in de-escalation, self-defense and response to emergency codes. When threatening language and agitation are identified, initiate de-escalation techniques quickly. – – Self-defense training may include topics such as violence risk factors, de-escalation techniques, alarms, security support, safe rooms, escape plans, and emergency communication procedures. Regarding de-escalation and self-defense, experts suggest that hospitals prohibit firearms from campus, except for firearms used by law enforcement officers. – – Conduct practice drills that include response to a full spectrum of violent situations, which could range from a verbally abusive family member to an active shooter.”
In their 2015 Guidelines, OSHA says this on page 24:
“Education and training are key elements of a workplace violence protection program, and help ensure that all staff members are aware of potential hazards and how to protect themselves and their co-workers through established policies and procedures. Such training can be part of a broader type of instruction that includes protecting patients and clients (such as training on de-escalation techniques). However, employers should ensure that worker safety is a separate component that is thoroughly addressed.”
In OSHA’s report, Caring for Our Caregivers December 2015, they say this on page 25:
“Training is a key component of a successful workplace violence prevention program. It helps healthcare workers learn to recognize potential hazards and learn how to protect themselves, their coworkers, and their patients. Training and reinforcement through role-playing and other means can provide employees with strategies that increase their confidence for handling potentially violent incidents before they arise and reduce the likelihood of violent incidents occurring. Education also reinforces that violence is not an acceptable part of healthcare work.”
The OSHA Guidelines go on to recommend these specific elements of an effective WPV safety and health training program:
- Involve all workers, including visiting staff, contract workers, supervisors, and managers
- Provide special instruction for workers who face specific safety and security hazards
- Teach the concept of “universal precautions for violence” (violence should be expected but can be avoided or mitigated through preparation)
- Communicate the importance of a culture of respect, dignity, and active mutual engagement in preventing workplace violence
- Instruct at the comprehension level appropriate for the staff — using qualified instructors
- Cover policies and procedures as well as de-escalation and self-defense techniques
- Use role-playing, simulations, and drills
- Train new workers before beginning their job duties, train all workers at least annually, and in high-risk settings, train quarterly or even monthly
Relative to topics to be covered in a WPV safety and health training program, the OSHA Guidelines say this on 25 and 26:
“Training topics may include management of assaultive behavior, professional/police assault-response training, or personal safety training on how to prevent and avoid assaults. A combination of training programs may be used, depending on the severity of the risk. In general, training should cover the policies and procedures for a facility as well as de-escalation and self-defense techniques. Both de-escalation and self-defense training should include a hands-on component.”
And here are some of the topics OSHA suggest be covered:
- Workplace violence prevention policy
- Risk factors that cause or contribute to assaults
- Recognition of escalating behavior, warning signs, or situations that may lead to assaults
- De-escalation techniques which can be used to prevent or diffuse volatile situations or aggressive behavior
- Approaches to deal with aggressive behavior in people other than patients and clients, such as relatives, visitors, or intruders
- Self-defense procedures where appropriate
- Ways to protect oneself and coworkers, including working in teams when necessary
- Policies and procedures for reporting and record-keeping
Here are a few additional points OSHA makes about an effective WPV safety and health training program:
- Train all workers who are reasonably expected to interact with patients, including admissions staff
- Training programs are most effective when they are designed specifically for a facility or unit’s particular risk profile. Also, because duties, work locations, and patient interactions vary by job, violence prevention training can be more effective if it is customized to address the needs of different groups of healthcare personnel. For example:
- Provide direct caregivers with training tailored to the specific patient population with which they work — such as behavioral health patients, the developmentally disabled, and geriatric patients with Alzheimer’s and other forms of dementia
- Specialized training for ED staff with a focus on the most common threats faced at their facility (using such resources as those available from the Emergency Nurses Association)
- Specific training for security personnel, including the psychological components of handling aggressive and abusive clients, and ways to handle aggression and defuse hostile situations
- Separate training for housekeeping, food service, maintenance, and other support staff
- Training and policies should cover all types of workplace violence, not just violence by patients against employees (e.g., employee-on-employee violence, employee-on-patient violence
- Interactive exercises make training more effective by allowing participants to practice and apply the skills they have learned, such as de-escalation and self-defense techniques
- Web-based training offers fidelity of presentation and automated documentation while requiring minimal supervision and allowing flexible timing and pace. Web-based training may be more effective when paired with live instruction and practice (blended training)
- It can be helpful to have a team of trained WPV prevention trainers in-house. One option is for employees to attend a more in-depth course offered by an outside training provider to become certified to train others within their organization
- Another approach is to have one or more “safety coaches” for each unit or floor to offer guidance and coaching in real-time and to run ad hoc refresher sessions
Again, OSHA cannot cite a healthcare organization for not having a WPV safety and health training program. However, they can cite an organization if 1) they identify “hazards that are causing or likely to cause death or serious physical harm to employees” 2) they can show that some action could have been taken to materially reduce the hazards.
Obviously, having a strong WPV program in place reduces the chances that OSHA would make such a determination during an inspection as a result of an employee complaint about workplace violence.
Vistelar’s Alignment With Joint Commission and OSHA
As stated earlier, the above review provides a foundation for Vistelar’s recommendations relative to developing an effective WPV safety and health training program — the fourth building block specified in OSHA’s Guidelines for Preventing Workplace Violence for Healthcare and Social Server Workers – 2015.
Obviously, it is important to follow the Joint Commission’s and OSHA’s published guidelines to provide protection from an OSHA citation and in anticipation of OSHA developing a workplace violence standard for healthcare settings. In addition, in Vistelar’s opinion, these guidelines are sound and practical in terms of protecting the safety and well-being of employees, patients, and visitors.
Although these guidelines for an effective WPV safety and health training program are relatively new, Vistelar’s trainers have identified and embraced most of the recommended elements for over thirty years. The following are just a few examples of the alignment of Vistelar training programs with the published guidelines of the Joint Commission and OSHA.
- Offer programs that address the entire spectrum of human conflict — non-escalation, de-escalation and crisis intervention coupled with physical alternatives (personal protection, self-defense, and defensive tactics — including active shooter preparation and response). Vistelar trains individuals and teams to prevent and better manage conflict — from simple disagreements to physical violence.
- Address all the topics suggested by OSHA (plus more — see below) which cover all types of workplace violence (patient-on-employee, employee-on-employee, and employee-on-patient violence). We train on how to:
- Maintain safety when presented with a conflict situation
- Predict and prevent conflict
- De-escalate anger and abuse
- Control crisis and aggression
- Effectively manage physical violence
- Provide a spectrum of programs — web-based programs for admissions and support staff (“gatekeepers”), in-person and blended training workshops for direct caregivers, specialized programs for high-risk areas (e.g., ED, behavioral health) and security professionals, and instructor schools (train-the-trainer programs) for organizational instructors and “safety coaches.”
- Customize programs to meet our clients’ specific needs to ensure our training aligns with their unique mission, vision, and values and that the learning provided by our training is more sustainable over time.
- Underscore the need for physical, organizational, legal and emotional safety (Vistelar’s P.O.L.E. acronym) — with the goal of enhancing customer satisfaction, improving employee safety and morale, preventing reputations from being destroyed, reducing liabilities and injuries, and saving lives.
- Teach the concept of “universal precautions for violence” (in Vistelar terms — conflict is inevitable but it can be effectively managed to prevent and mitigate violence). Over the years, we’ve learned that you can’t stop conflict from happening but you can manage it in order to keep everyone safer.
- Share Vistelar’s core principle of conflict management — “treat people with dignity by showing them respect.”
- Train using Vistelar’s “fire drill versus fire talk” approach, which includes an optimum blend of student interaction, scenario-based skill practice, memorable stories, and analysis of real-life events captured on video — instead of solely lecture-based training. Also, in most classes, we video- and audio-record student role plays to document that learning has taken place and to emphasize that, in today’s society, the likelihood of an interaction getting caught on camera is almost 100%. Finally, our physical alternatives training is almost entirely hands-on.
- Emphasize a tactic Vistelar calls “Closure,” which we define as “follow-through considerations, such as ensuring the situation is stabilized, summarizing decisions, and reviewing the interaction.” The goals of this tactic are to achieve the best possible outcome, to end the interaction in a better place than where it started, and to establish a positive foundation for all future interactions. Incident reporting is strongly emphasized during coverage of this tactic.
Vistelar’s Additional Recommendations
Vistelar has developed additional recommendations based on our 30-plus years of training all levels of employees in a wide range of healthcare settings (e.g., hospitals, residential treatment, clinics, community care, home care) — as well as law enforcement professionals — beyond what the Joint Commission and OSHA recommends for an effective WPV safety and health training program,
Most of these recommendations are based on Vistelar’s Point-Of-Impact Conflict Management Framework™ (“6 C’s of Conflict Management”).
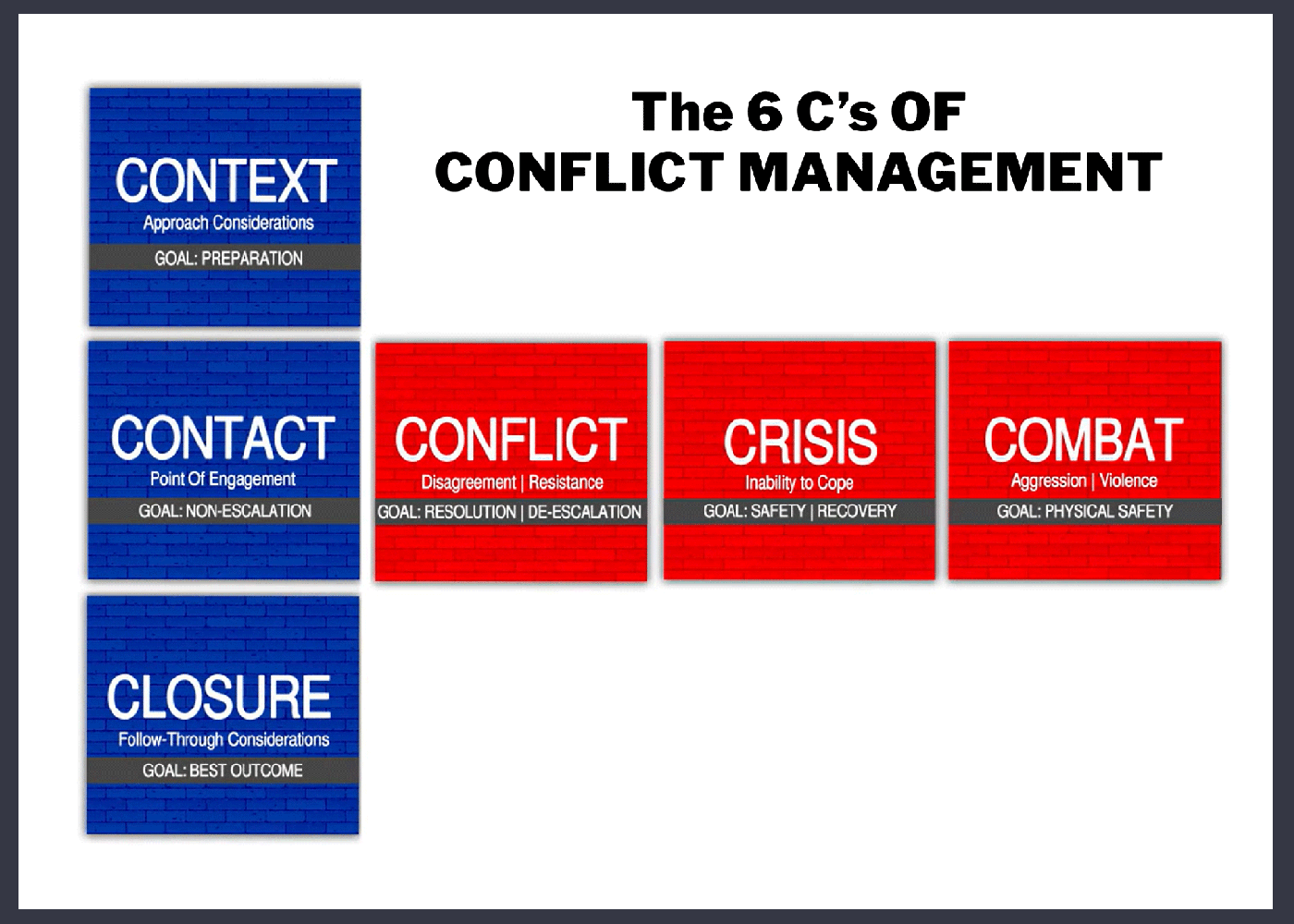 Note that this graphic has blue boxes (“blue brick road”) and red boxes (“red brick road”). Vistelar’s training emphasizes keeping people on the “blue brick road.” However, sometimes people take us on the “red brick road,” inflicting various levels of emotional and physical violence. When that happens, Vistelar’s training teaches how to bring people back to the “blue brick road,” with the goal of producing the best possible outcome.
Note that this graphic has blue boxes (“blue brick road”) and red boxes (“red brick road”). Vistelar’s training emphasizes keeping people on the “blue brick road.” However, sometimes people take us on the “red brick road,” inflicting various levels of emotional and physical violence. When that happens, Vistelar’s training teaches how to bring people back to the “blue brick road,” with the goal of producing the best possible outcome.
As represented by the orange and red jagged bars, there are two types of conflict: non-violent and violent — and it’s critically important to recognize that violent conflict is a possibility in every healthcare setting.
In addition, while uncomfortable to some, Vistelar uses the term “Combat” as a means to emphasize that physical engagement is a possibility in all jobs and must not be glossed over in conflict management training.
That is why Vistelar’s training programs “address the ENTIRE spectrum of human conflict” — meaning we cover all six elements of the conflict management framework.
- Context: Approach considerations prior to an interaction, such as assessment of risk and physical positioning, decision on whether to proceed, and personal mindset
- Contact: Interaction considerations, such as words used, tone of voice, facial expressions, eye contact, hand position, body language, and posture
- Closure: Follow-through considerations, such as ensuring the situation is stabilized, summarizing decisions, and reviewing the interaction
- Conflict: When questioning, anger or verbal abuse enters into an interaction
- Crisis: When the person with whom you are interacting is displaying at-risk behaviors
- Combat: When resistance or aggression results in physical engagement initiated by either party
In other words, Vistelar’s additional recommendations for an effective WPV safety and health training program are almost all related to ensuring the program doesn’t lead to employees having their “training tape run out” when faced with an uncommon situation.
For example, we recommend that all employees get at least some training on how to respond in the face of violent crisis intervention or physical engagement (a tactic we call “Take Appropriate Action”).
Note: Vistelar’s expertise in dealing with violent crisis and physical violence stems from our founders’ 30-plus years of field-proven law enforcement and military experience. In fact, throughout the 80s and 90s, one of our founders helped develop Wisconsin’s nationally recognized unified tactical training systems (D.A.A.T and P.O.S.C®). Every police officer, jail/juvenile detention officer and prison/probation/parole officer is trained in one of these systems.
Another example is that we recommend training on two tactics we call “Be Alert & Decisive – Respond, Don’t React” and “Proxemics 10-5-2,” which emphasize personal safety awareness and the use of distance, relative positioning and hand placement to stay safe.
A third example is that we devote significant time in class to perspective taking — how to demonstrate empathy to another person’s situation. Perspective taking is the basis of our emphasis on “non-escalation,” preventing conflict to minimize the chance that simple disagreements will escalate to emotional and/or physical violence.
In general, our additional recommendations, are focused on ensuring your organization’s safety and health training programs embed in students the knowledge, skills, and abilities to interact with anyone and to:
- Engage in a way to not cause conflict or unnecessarily escalate situations
- Confidently and professionally deal with questioning, anger, and verbal abuse
- Participate in difficult conversations and mediate positive outcomes
- Effectively de-escalate conflict and remain safe in crisis situations
- Persuade others to cooperate in the face of resistance
- End an interaction in a better place than where it started
- Know what to do and how to do it when resistance or aggression results in physical engagement
- Defend oneself from a physical assault
- Take appropriate action (e.g., exit, evade, escape, stabilization, control) based on the employee’s role within the organization and their training and experience, the environment they are in, established policies and procedures, availability of security or police, and defined rules of engagement
- If necessary, articulate a legal defense for taking appropriate action
Conclusion
Workplace violence is a significant problem in healthcare settings as evidenced by 65% of OSHA complaints involving the healthcare industry. In order to support the safety of employees, patients, and visitors and to protect themselves from OSHA citations, healthcare organizations should put in place a strong WPV prevention program.
One element of such a program should be an effective WP safety and health training program which follows the published guidelines of the Joint Commission and OSHA.
This report summarizes those guidelines and offers additional recommendations based on Vistelar trainer’s 30-plus years of experience in providing training in healthcare to address the entire spectrum of human conflict — non-escalation, de-escalation, and crisis intervention coupled with physical alternatives.